RICHARD R. HEUSER, MD, FACC, FACP, FESC, FSCAI 
Chief of Cardiology, St. Luke’s Medical Center, Phoenix, AZ
Professor of Medicine Univ. of Arizona, College of Medicine, Phoenix, AZ

AJAY U. MHATRE, MD
MICHAEL MAKKI, DO
SINA NAFISI, MD
This blog post discusses the symptoms, diagnostic imaging and treatment of May-Thurner Syndrome. May-Thurner syndrome (MTS) is a rarely diagnosed condition occurring when the left iliac (leg) vein is compressed by the right iliac artery. This condition increases the risk of deep vein thrombosis (DVT) in the left extremity. If you have concerns about your current heart health please call the Phoenix Heart Center to schedule an appointment today.
In 1851 Virchow observed that iliofemoral deep venous thrombosis (DVT) occurred five times more often on the left leg compared to the right. May and Thurner provided an explanation of this phenomenon by discovering an anatomical variation of the left common iliac vein in 1957. They found that the left common iliac vein had vascular thickening at the point where it was crossed and compressed against the fifth lumbar vertebrae by the overlying right common iliac artery. They called this a “venous spur” and felt it was due to the chronic pulsation of the overlying iliac artery resulting in this venous obstruction. This anatomic variant later became recognized as the May-Thurner Syndrome (MTS) (1).
In August of 2016, a 66 year old woman came to the Phoenix Heart Center with a history of periodically swollen legs for at least 20 years. While she admitted to having occasional right leg pain, she did not have any history of inflammation or blood clots in the lungs. During her examination, Dr. Heuser noticed she had mild swelling in her ankle and mild varicose veins in both inner thighs. The patient was told she had left renal vein varicosities noted on imaging in the mid-80s. She had bilateral great and smaller saphenous vein severe reflux. Her varicosities noted made Dr. Heuser and his team concerned about whether she had venous obstructive disease. To examine further, Dr. Heuser performed a venography with bilateral intravascular ultrasound examination. The diagnostic images can be seen below.

This venogram (or dye test) shows some mild narrowing present on the right iliac (leg) vein. Notice the intervascular ultrasound image (below) shows much more severe narrowing.
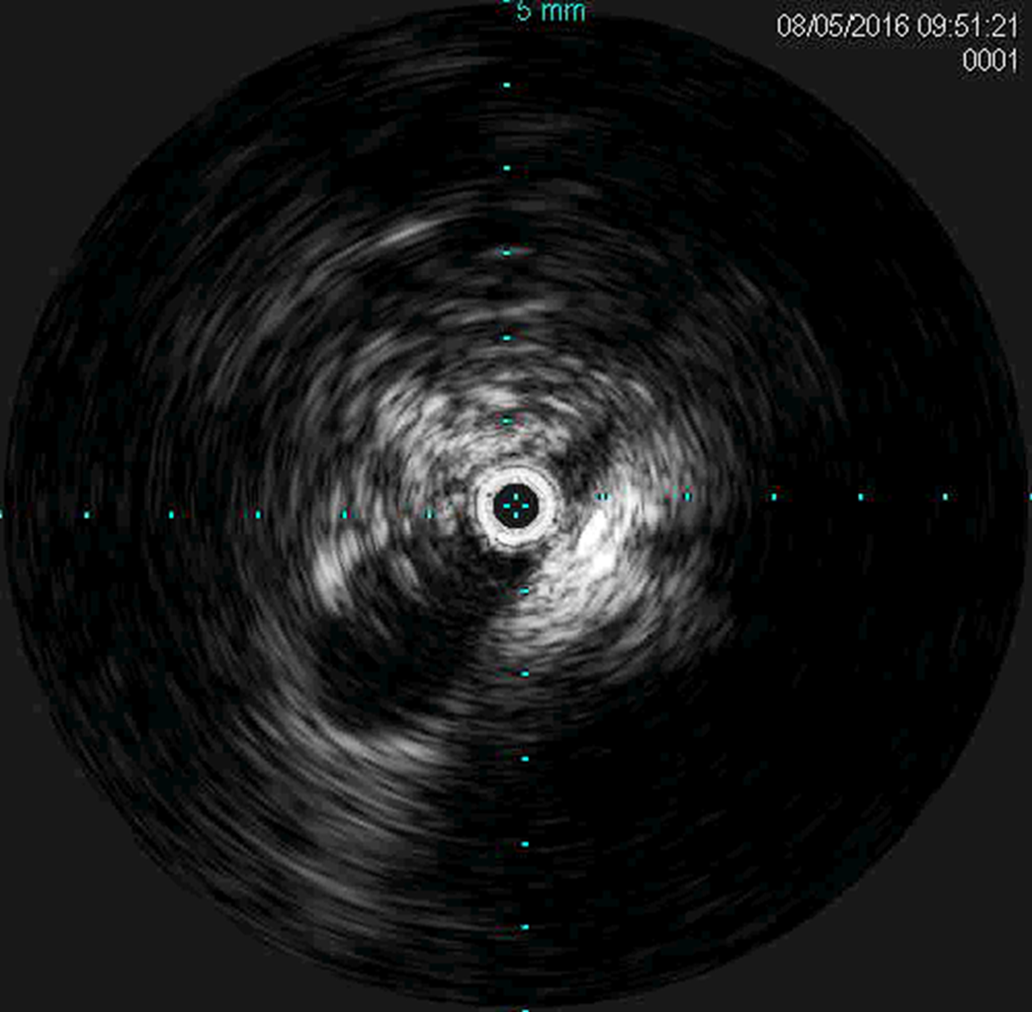
An ultrasound of the right iliac vein shows that there is only a small slit of blood flow. The white surrounding area is fibrous or scar tissue compressing the vein due to the iliac artery compressing this structure.

This venogram on the left side shows many collateral branches and impingement of the iliac vein due to the overlying iliac artery.
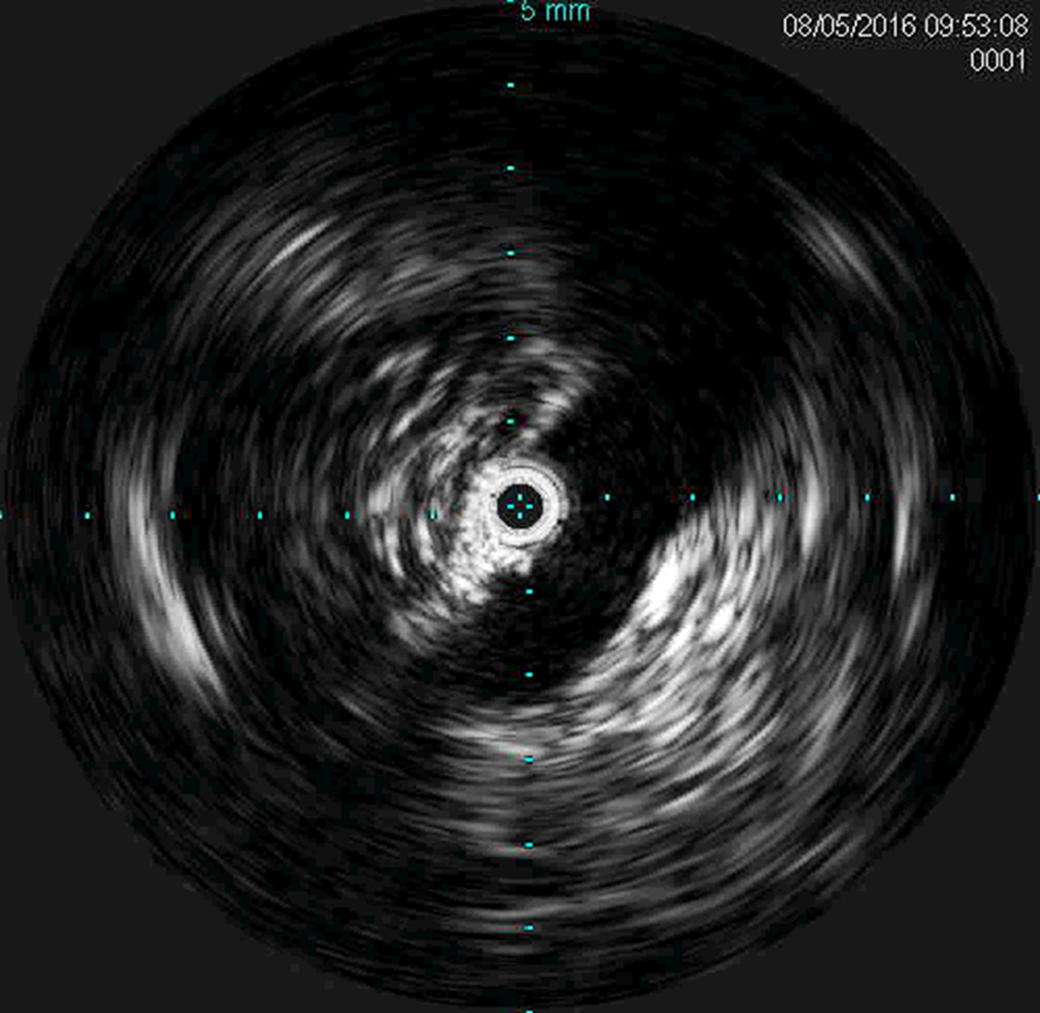
The left iliac vein also shows compression due to the overlying artery. This is typical in the May-Thurner Syndrome.

A balloon is expanded on the left side showing impingement or narrowing at the site of the iliac vein narrowing.

Left venogram after placement of the iliac vein stent.

This x-ray view shows the placement of the two iliac vein or leg vein stents relieving the obstruction.
The true occurrence of May-Thurner Syndrome is unknown and may range from 22-32% (2, 3). The syndrome is usually seen in females in the age group of 20-40 years of age and is thought to account for only 2-3% of all lower extremity DVTs. Continued trauma will lead to local extensive intimal proliferation resulting in impaired venous return; however, unlike in other patients, this did not result in venous thrombosis in our patient. It is also possible that the patient was suffering from a non-occlusive iliac vein lesion. MTS usually refers to left iliac vein compression. Although it’s rare, MTS can also be right sided and even more unusual, bilateral. Bilateral vein compression can be the result of uterine fibroids, tortuous iliac arteries or a pelvic mass.
Conclusion
May-Thurner Syndrome continues to challenge medical practitioners today. Just like it is important to think of MTS as a differential diagnosis in patients with unilateral DVT, in patients with leg swelling and perhaps before treating the lower leg venous reflux with surgery, it’s best to perform evaluation to rule out blockage in the veins. A venographic phase of an arterial CTA may also diagnose iliac compression. Diagnostic criteria are somewhat arbitrary, but before many operators would stent a symptomatic patient, the stenosis should be greater than 50%-60%. Our Phoenix Heart Center patient has done well in follow up and has had no further swelling or leg pain. With early recognition and aggressive management, May-Thurner Syndrome can be a well-managed disease.
References
- Kalu S, Shah P Natarajan A, Nwankwo N. May-Thurner Syndrome: A case report and Review of the Literature. Case Reports in Vascular Medicine. Volume 2013, Article ID 740182, 5 pages.
- R. May and J. Thurner, The cause of the predominately sinistral occurrence of thrombosis of the pelvic veins. Angioplasty 1957;Vol 8:419-427.
- M. R. Kibble, M. Ujiki, A. L. Goodwin, et al. Iliac vein compression in an asymptomatic patient population. J of Vasc Surgery 2004:Vol. 39(5); 937-943.
